1800 867 1390
1800 867 1390Case discussion: A 76-year-old female presents with a large ulcerating area on her neck. What would you do?

HealthCert Education
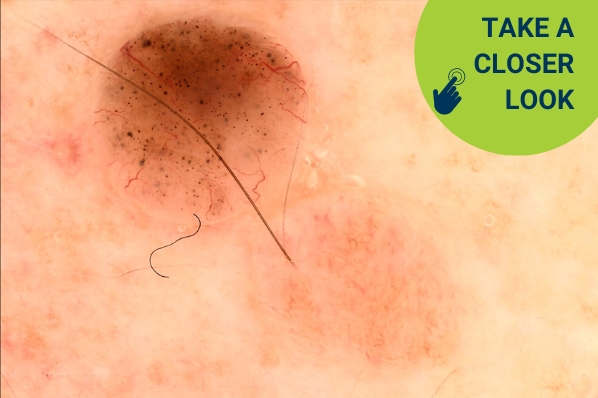
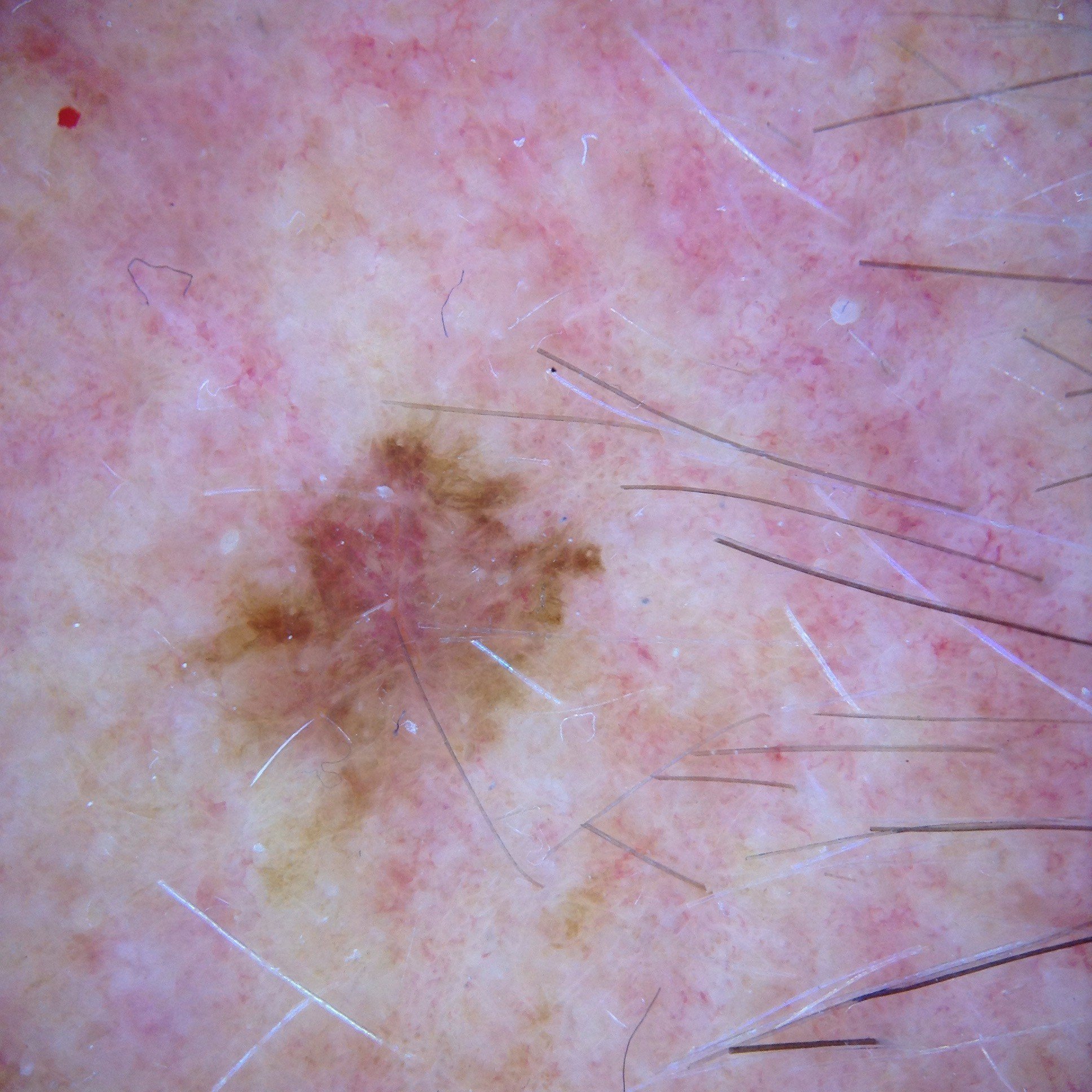
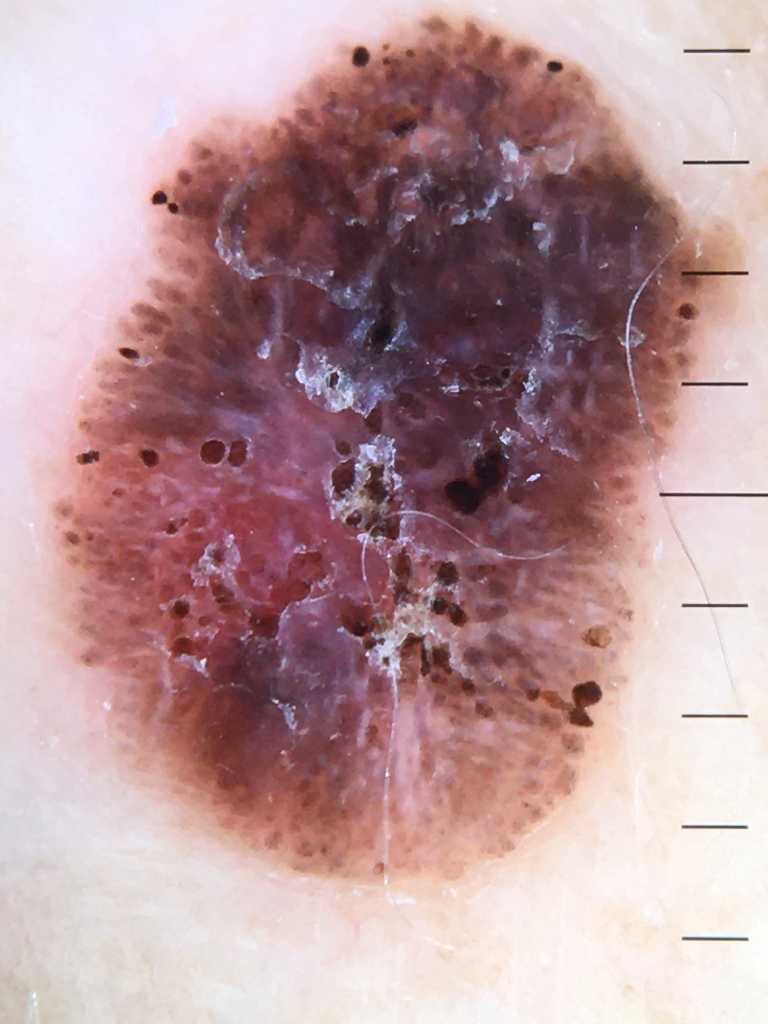
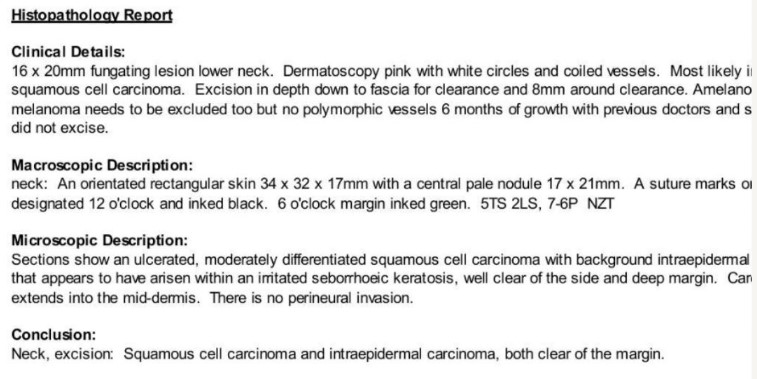
In this week’s case discussion, submitted by Dr Renuka Ranasinghe, we look at a 76-year-old female patient who presented with a large ulcerating area on her neck.
What is your diagnosis, and how would you manage this lesion?


Update
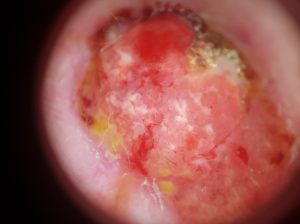
Here is the histopathology report (apologies for the cut-off edge), plus surgery photos.

For further information on this topic, you may be interested to learn more about the HealthCert Professional Diploma program in Skin Cancer Medicine.
 Would you like to share your experience with your colleagues in the weekly blog case discussion, moderated by Dr Terry Harvey?
Would you like to share your experience with your colleagues in the weekly blog case discussion, moderated by Dr Terry Harvey?
Participate with your cases so that we can learn together!
Submit your case here or send details to admin@healthcert.com