1800 867 1390
1800 867 1390Case discussion: 48-year-old male with elevated, firm and growing lesion on his right hand. Previous BCC excision adjacent to lesion. What would you do?

HealthCert Education
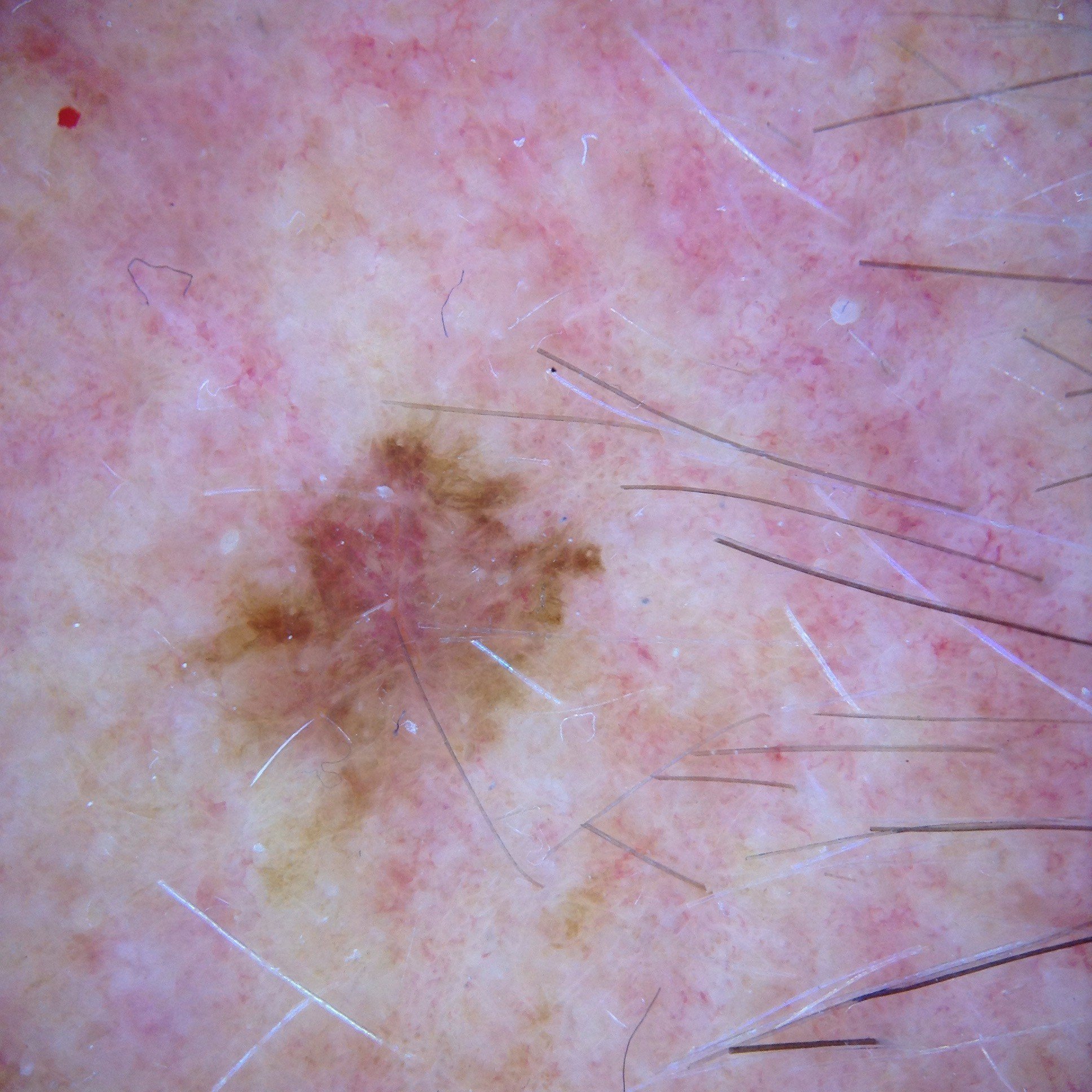
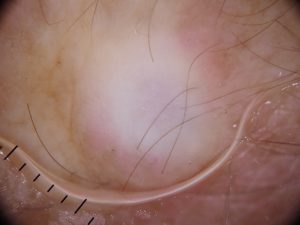
This week's case discussion, submitted by Dr Robert Teunisse, features a 48-year-old male patient with an elevated, firm and growing lesion on his right hand. There is a previous BCC excision adjacent to this lesion.
What do you think, and what would you do?


Update:
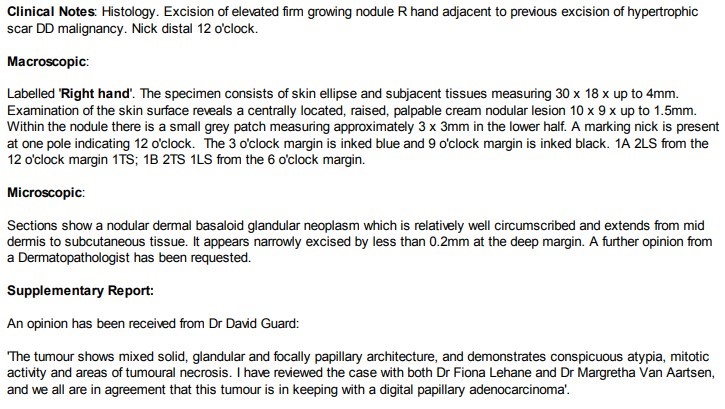
Here is the pathology report. The patient was referred to a local melanoma surgeon who did a wide local excision and lymph nodes from elbow and axilla.

Would you like to obtain advice or share your experience with your colleagues and Dr Terry Harvey in the weekly blog case discussion?
Participate with your cases so that we can learn together!
Submit your case here or send details to admin@healthcert.com