1800 867 1390
1800 867 1390Case discussion: 73-year-old male patient presents for full skin check. Pigmented lesion found on lower back. Patient has history of multiple melanomas.
HealthCert Education
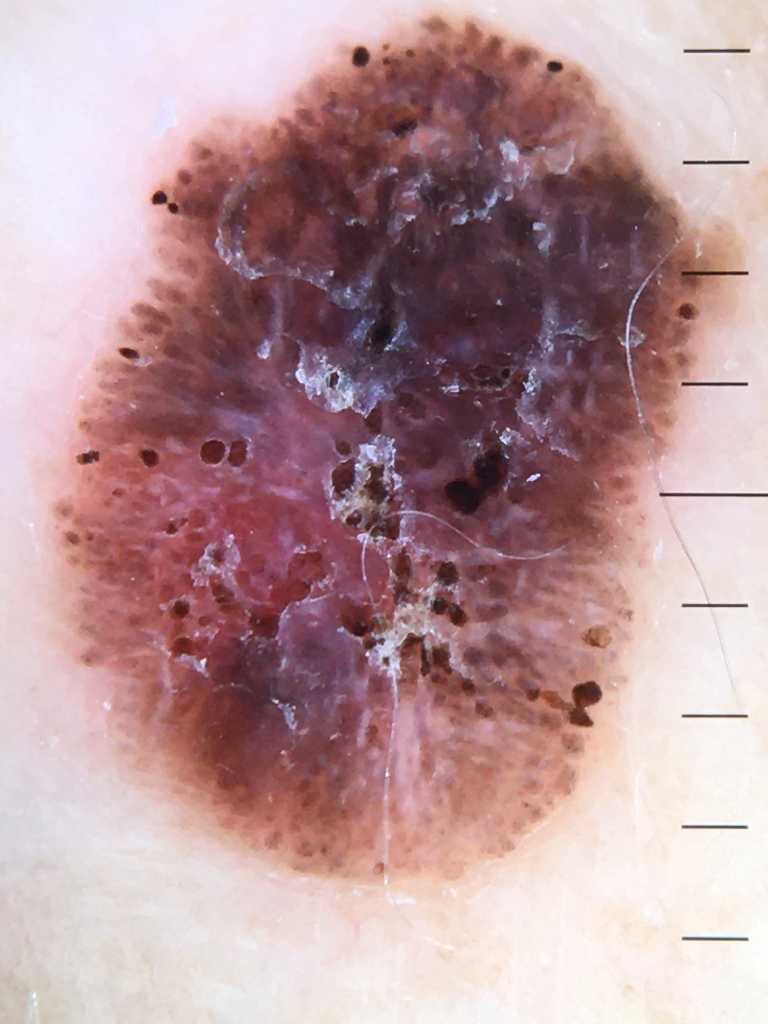
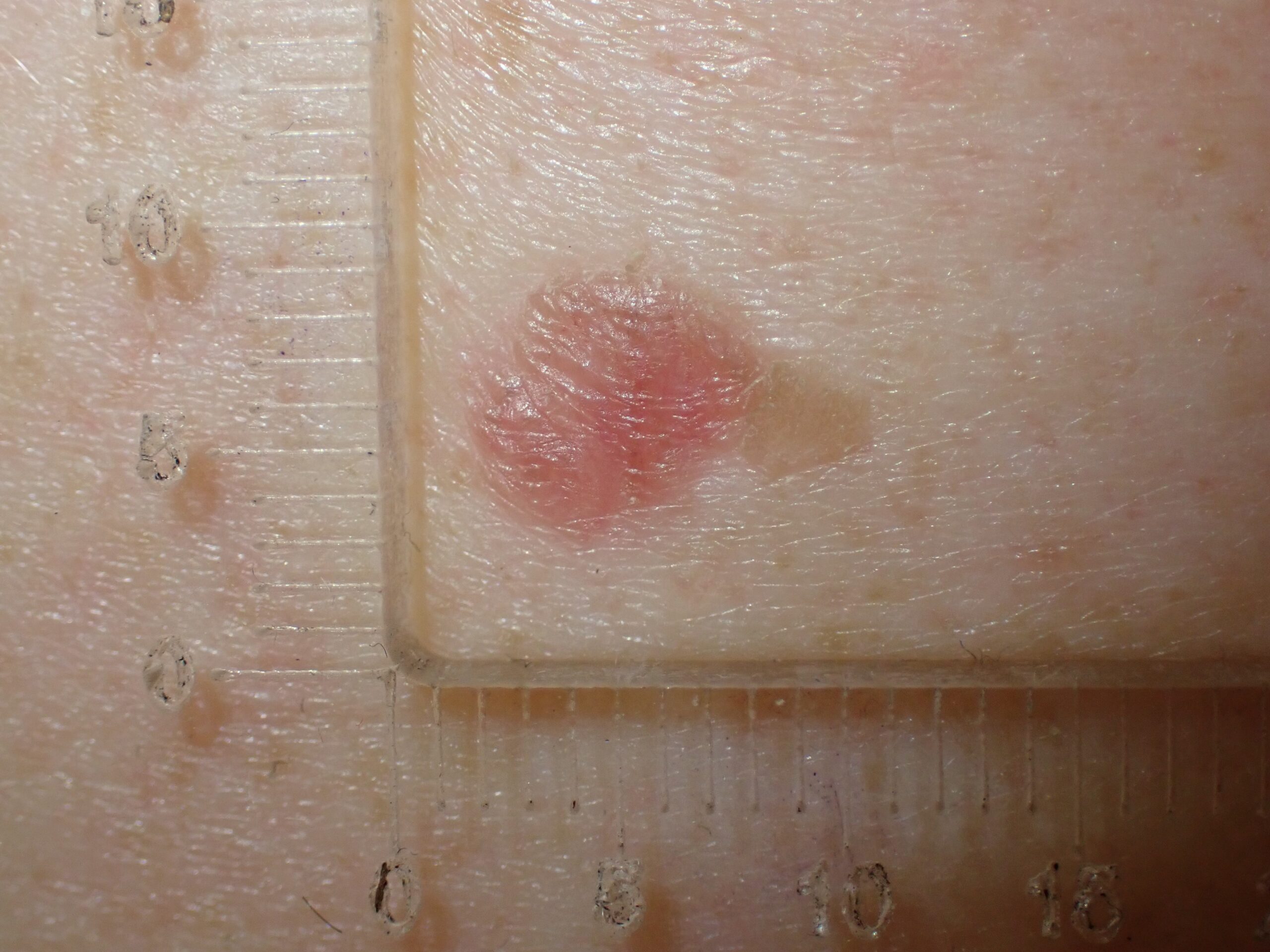
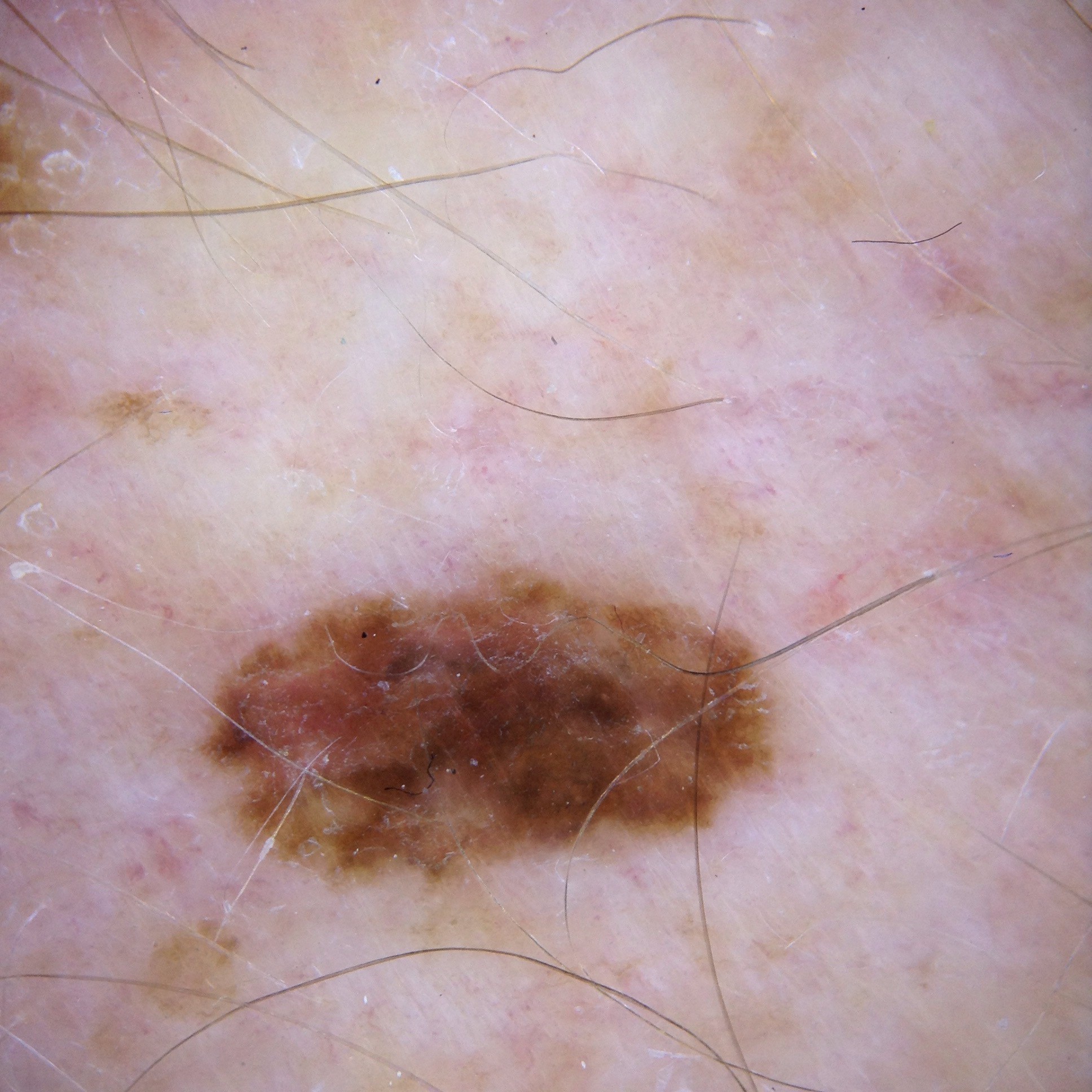
In this week's case discussion, submitted by Dr Magdy Malek, we look at a 73-year-old male patient who presented for a full-body skin cancer check and this pigmented lesion was found on his lower back. The patient has a history of multiple melanomas in the past.
What do you think of the dermoscopy, and what would you do?

Update
The lesion was shaved and histopathology revealed a Clark 2 melanoma with Breslow thickness 0.4mm. What next?

Would you like to obtain advice or share your experience with your colleagues and Dr Terry Harvey in the weekly blog case discussion?
Participate with your cases so that we can learn together!
Submit your case here or send details to admin@healthcert.com