1800 867 1390
1800 867 1390Cade discussion: 59-year-old female patient, no previous skin cancers, presented with lesion on arm, growing 2 years. What do you make of the dermoscopy?
Author
HealthCert Education
HealthCert Education
1 minute read
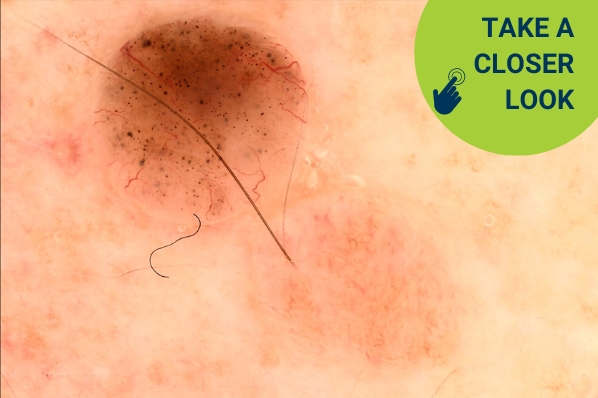
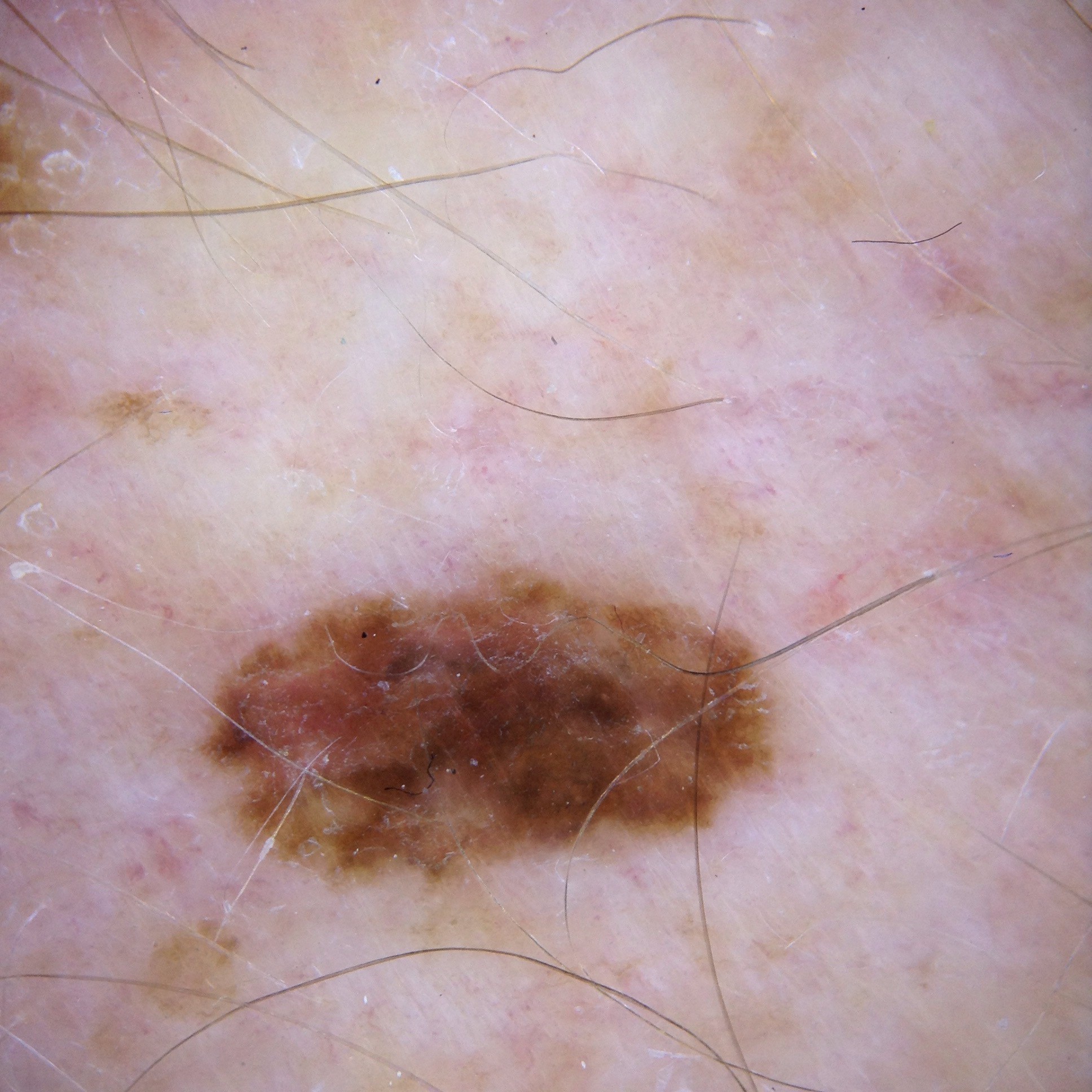
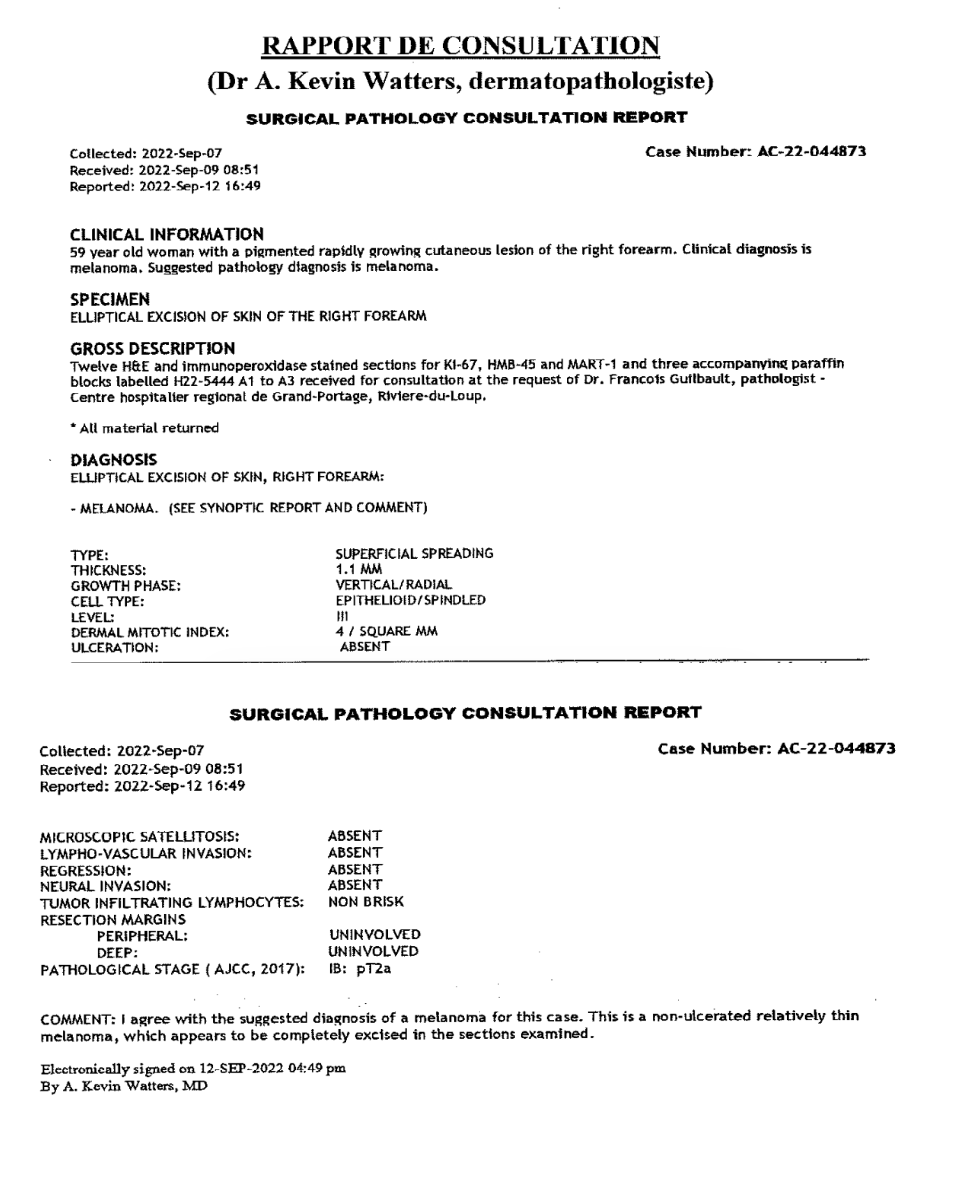
This week's case discussion from Dr Céline Bordeleau features a 59-year-old female patient with no previous skin cancers, who presented with a lesion on her right arm that had been present for two years and slowly growing.
What do you make of the dermoscopy?
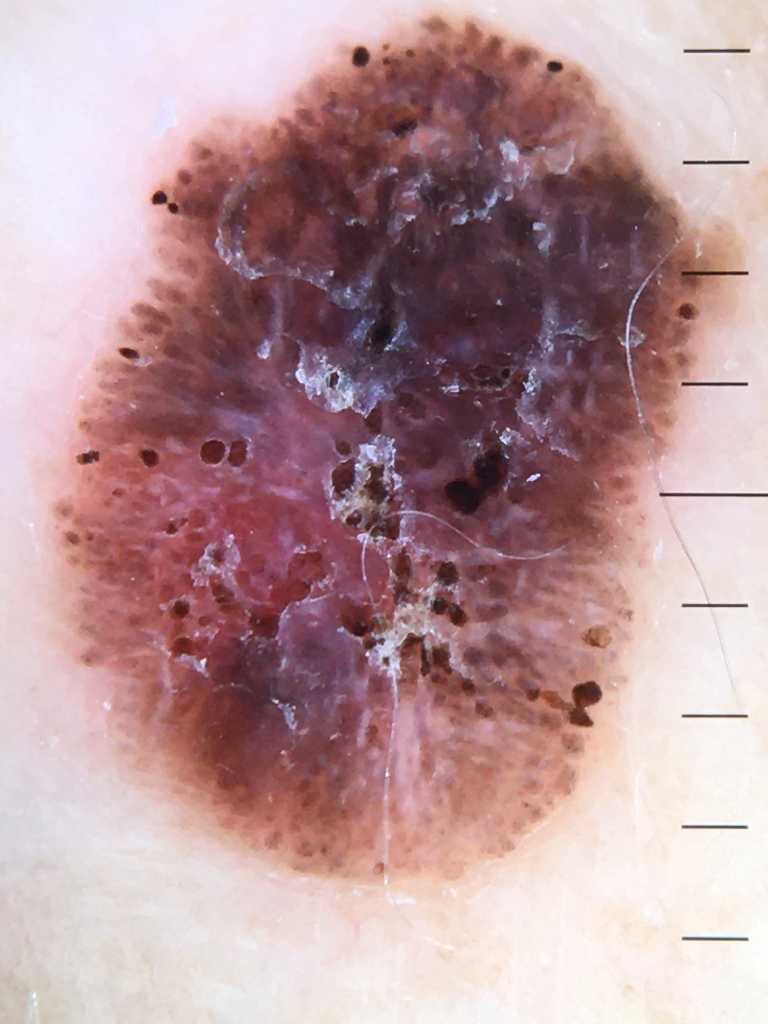
Update:
Here is the pathology. What next?

Would you like to obtain advice or share your experience with your colleagues and Dr Terry Harvey in the weekly blog case discussion?
Participate with your cases so that we can learn together!
Submit your case here or send details to admin@healthcert.com
Comments