1800 867 1390
1800 867 1390Case discussion: We look at a pigmented lesion the doctor found on his hand; he is concerned it is suspicious. What do you think and what would you do?

Author
HealthCert Education
HealthCert Education
1 minute read
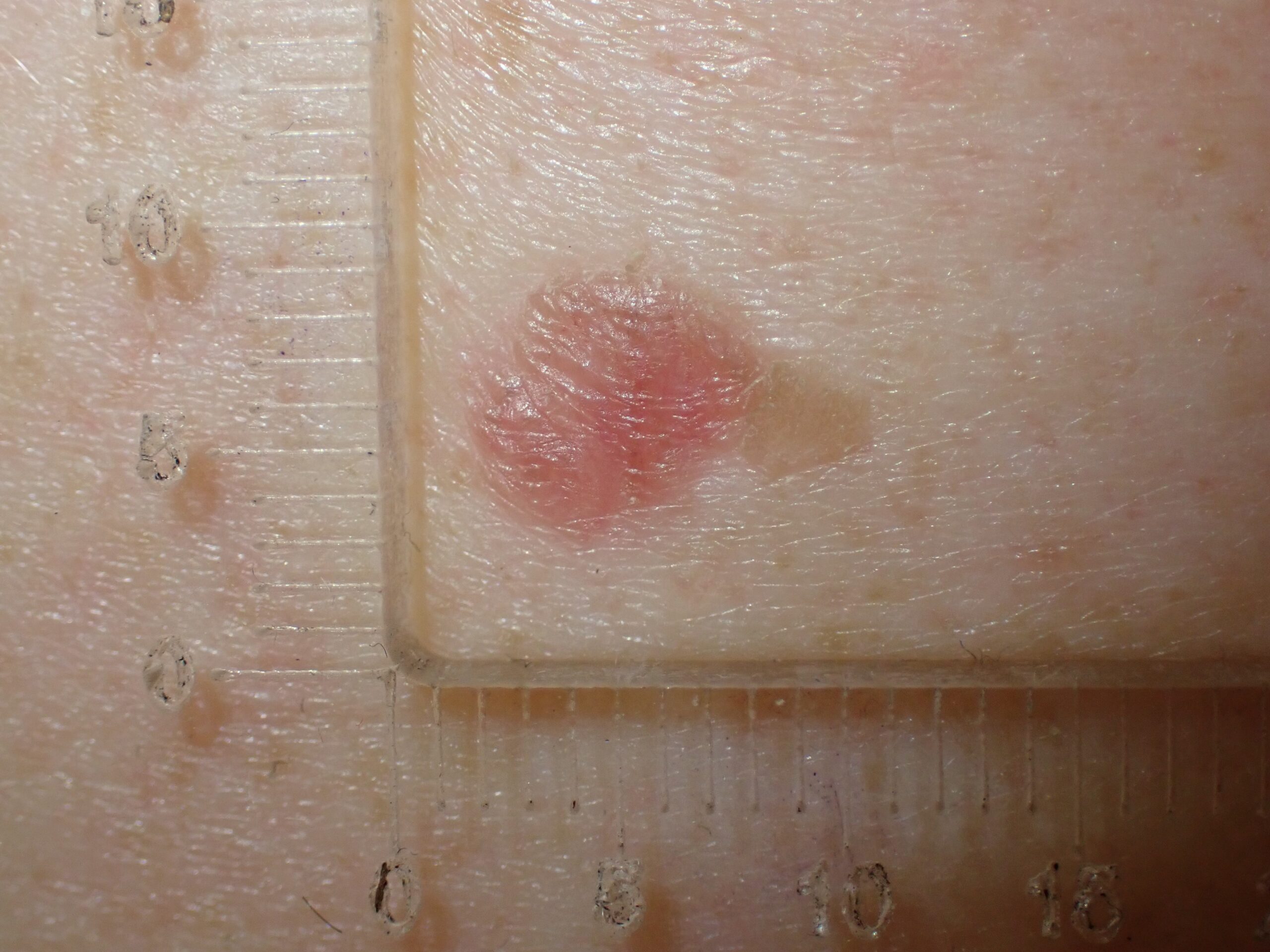
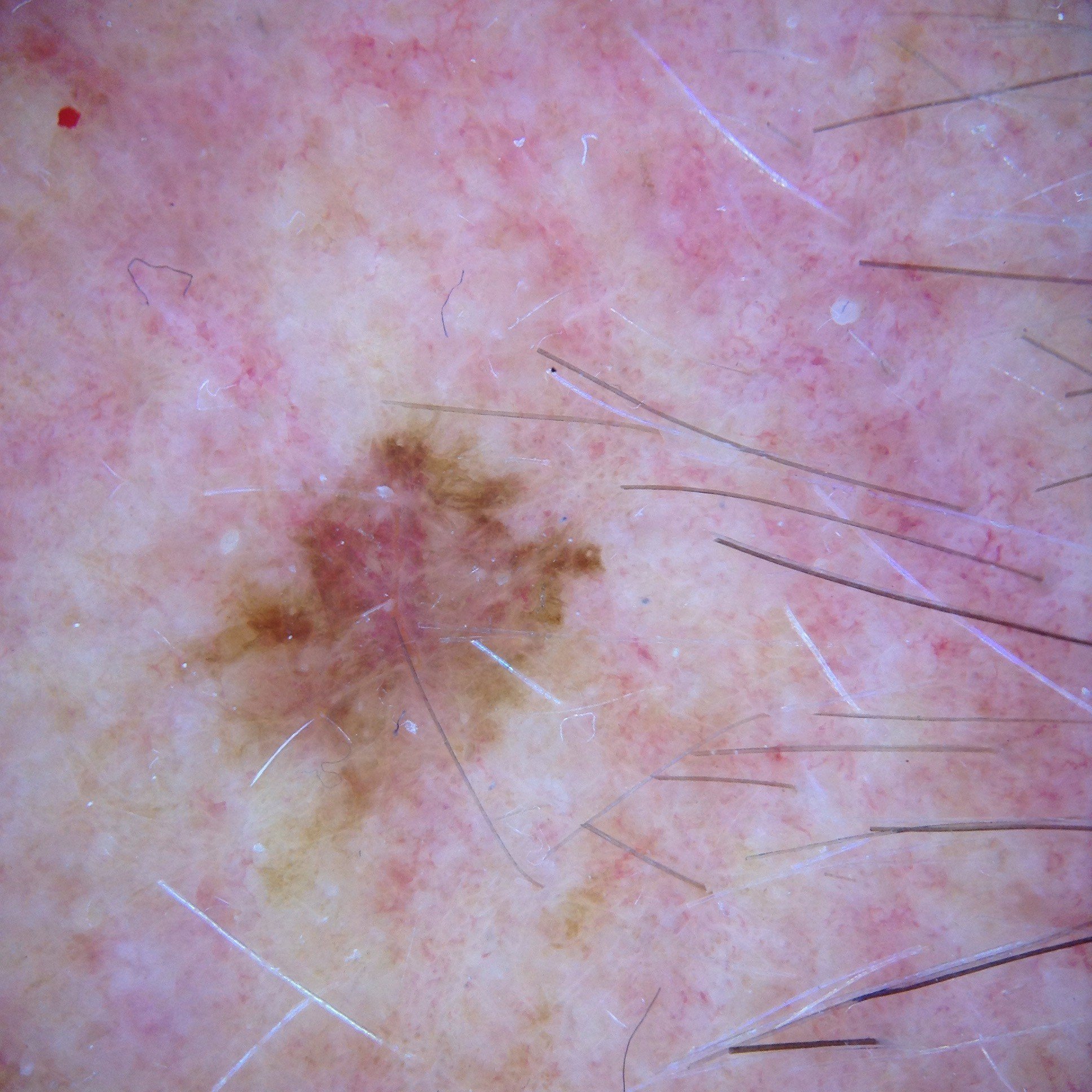
In this week's case discussion, we look at a pigmented lesion that Dr Ovida Vipulaguna found on his hand, and he is concerned it may be suspicious.
What do you think of the lesion and what would you do?


Update
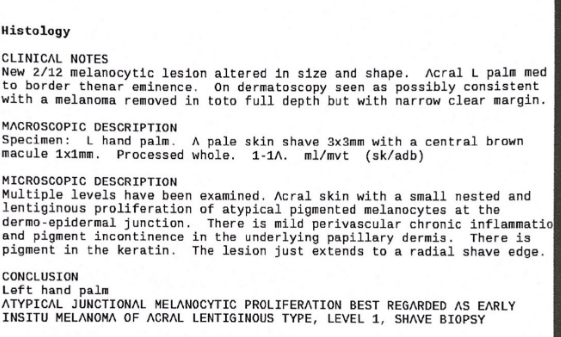
The result is below. What next?

Would you like to obtain advice or share your experience with your colleagues and Dr Terry Harvey in the weekly blog case discussion?
Participate with your cases so that we can learn together!
Submit your case here or send details to admin@healthcert.com
Comments