1800 867 1390
1800 867 1390Case discussion: An asymptomatic 70-year-old male presented for a total body skin exam. A small pink patch was noted. What would you do?
Author
HealthCert Education
HealthCert Education
1 minute read
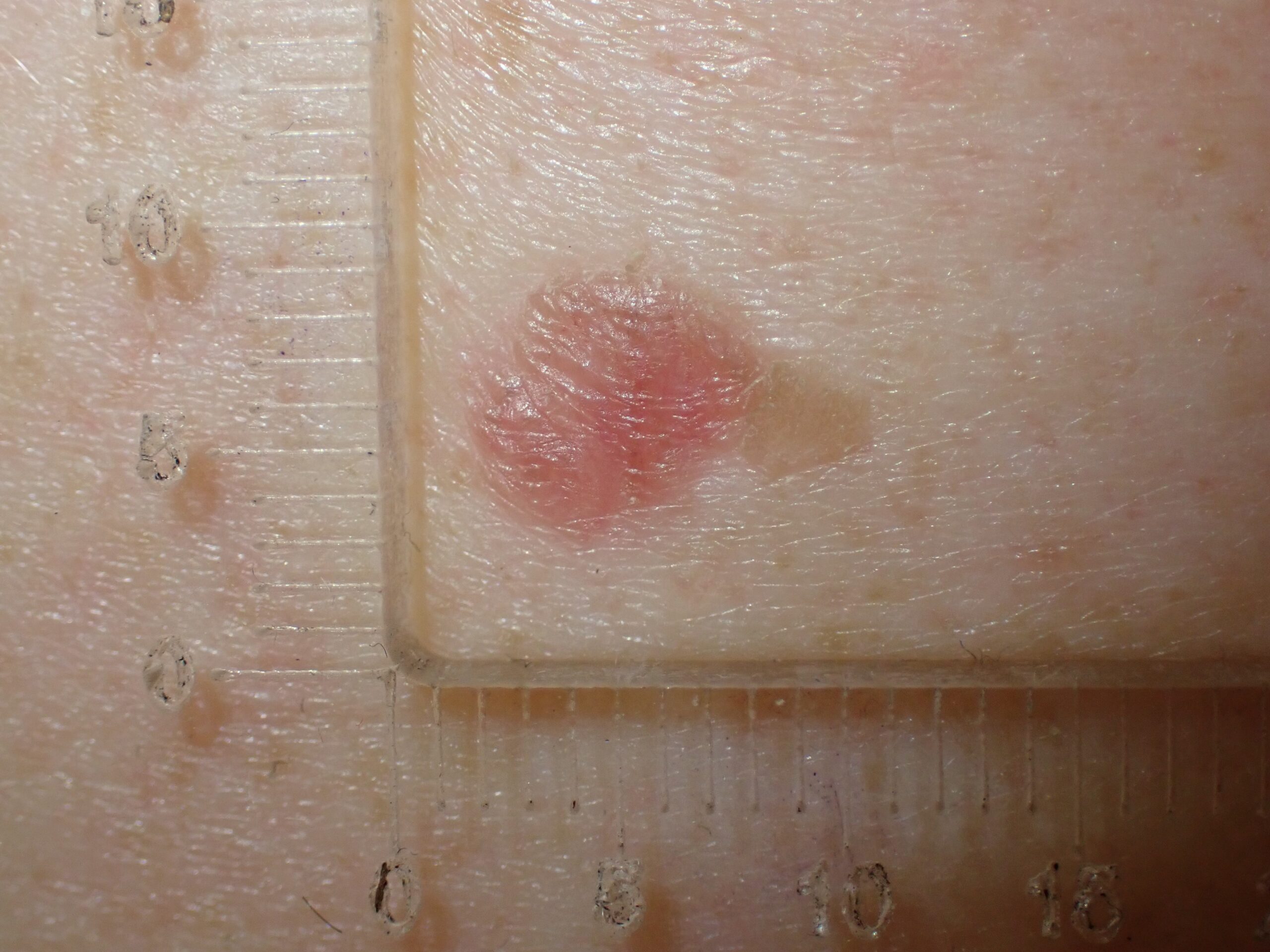
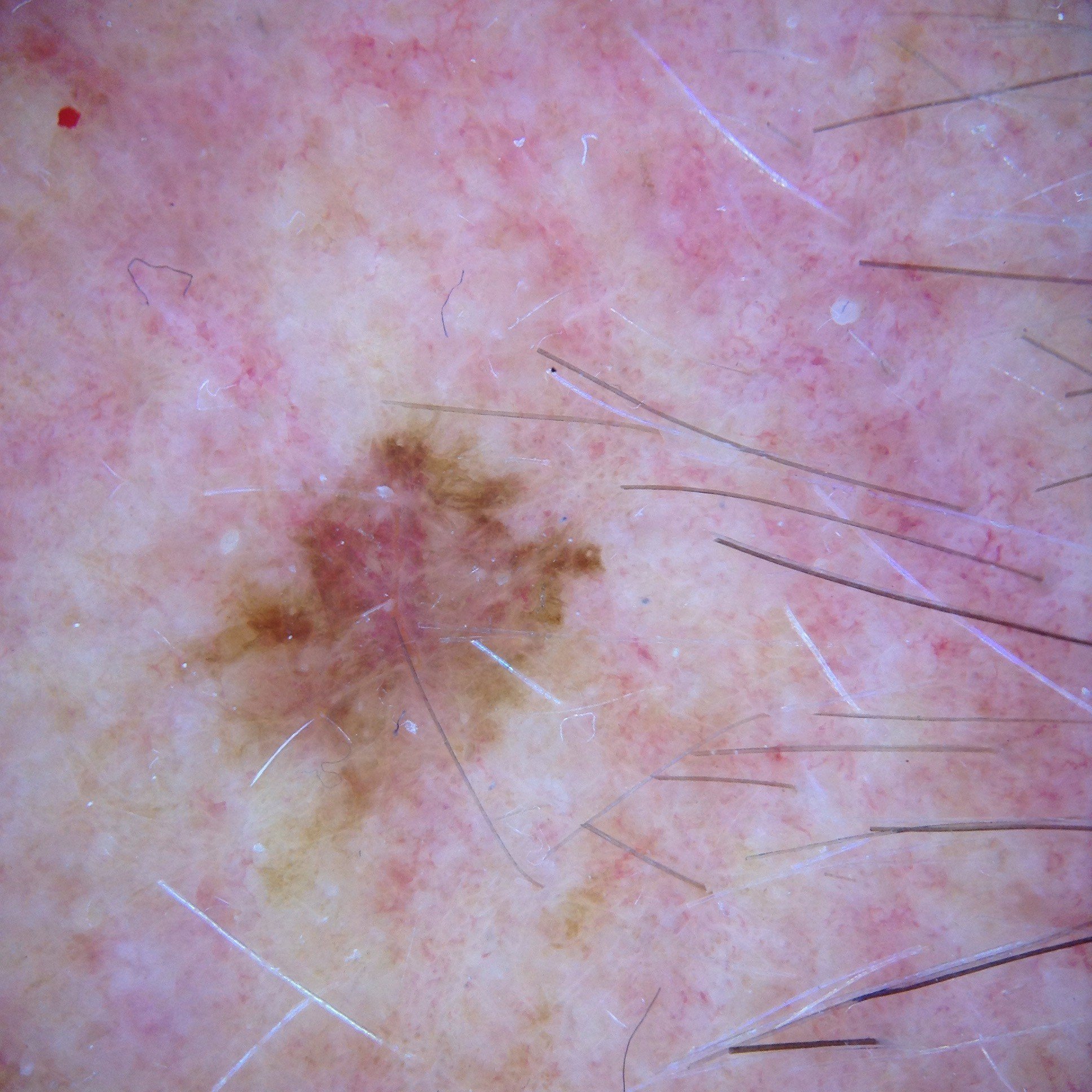
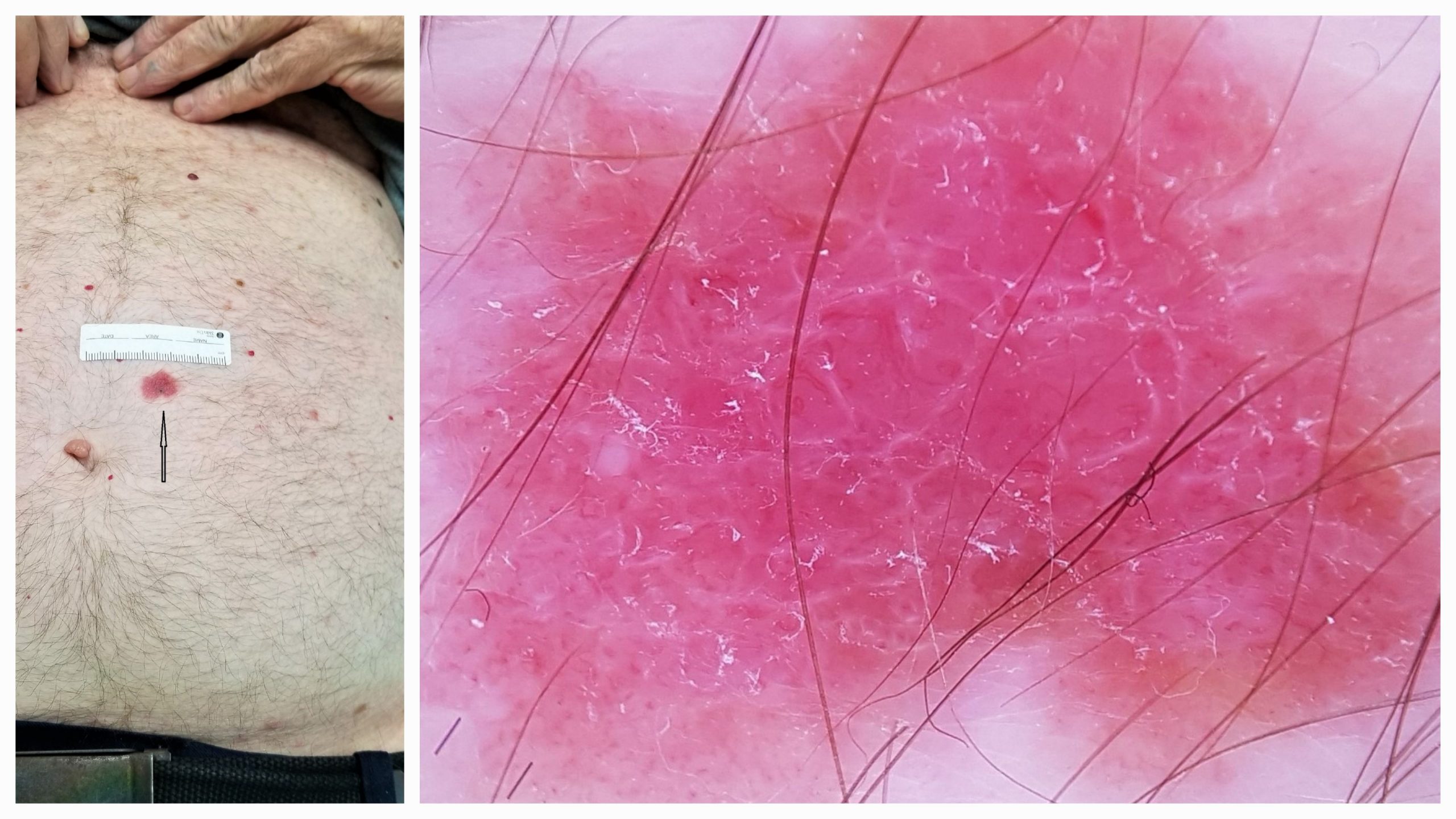
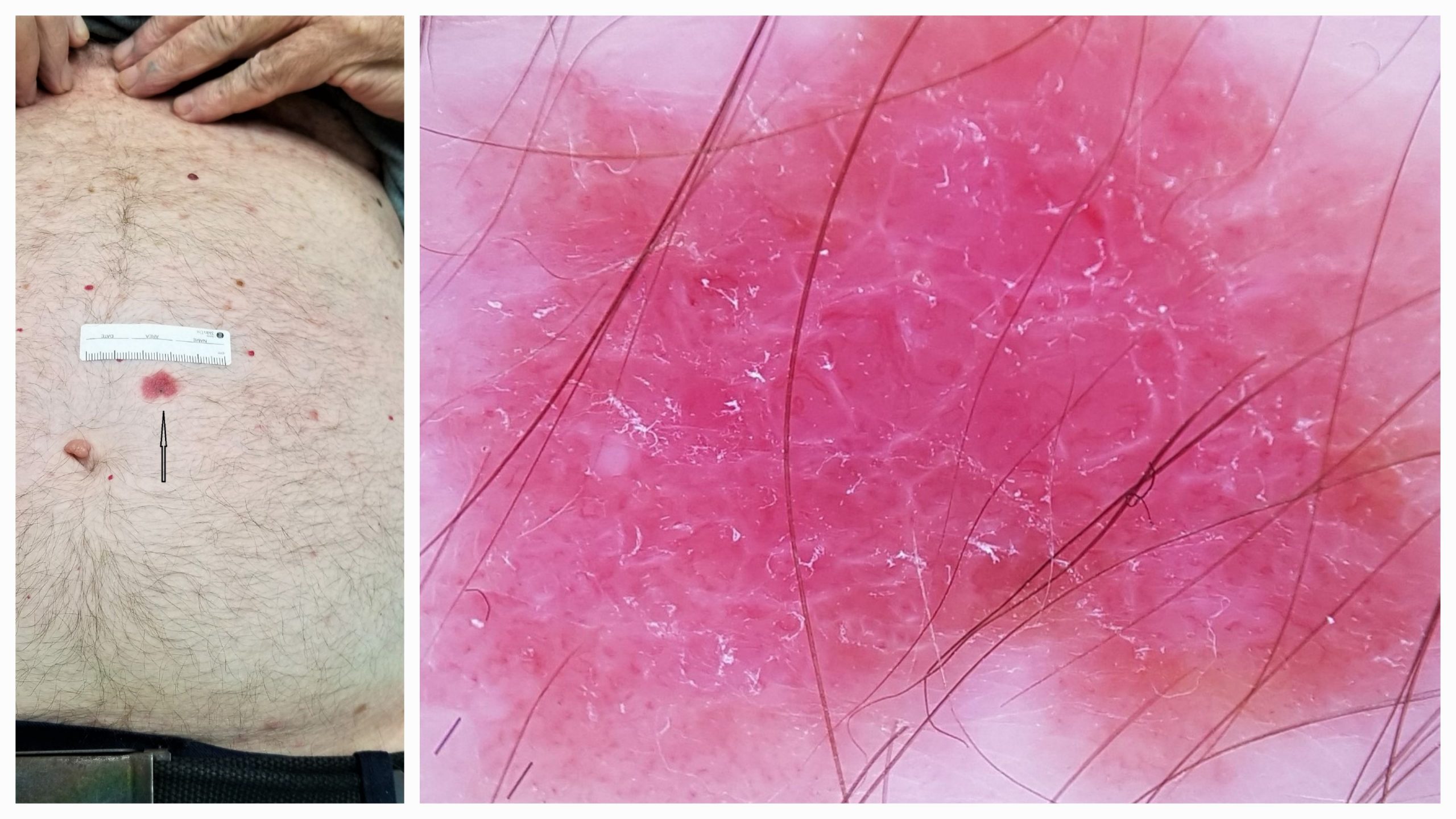
This week, we discuss an interesting case from Dr Tim Aung featuring an asymptomatic 70-year-old male who presented for a total body skin examination. A small pink patch was noted – see below images.
What do you think? What would you do?
Update
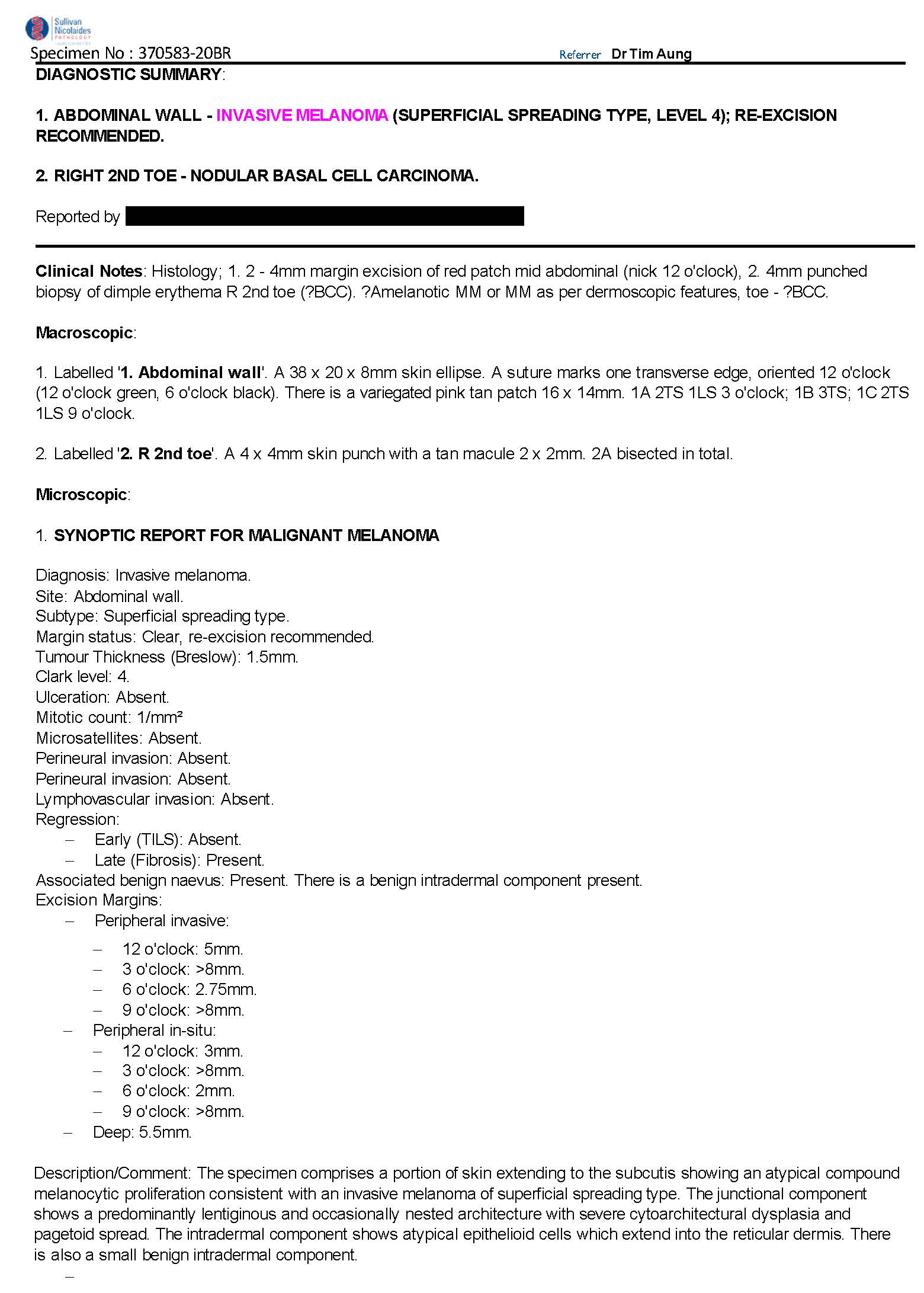
Here is the pathology report. What next?
– Prof David Wilkinson
We encourage you to participate in the case discussions and submit your own clinical images and questions, so we can all learn together.
Comments