1800 867 1390
1800 867 1390Case discussion: A 55-year-old female presented with 1-2 years' history of slow growth of an asymptomatic, non-tender lesion on the upper chest.
Author
HealthCert Education
HealthCert Education
1 minute read
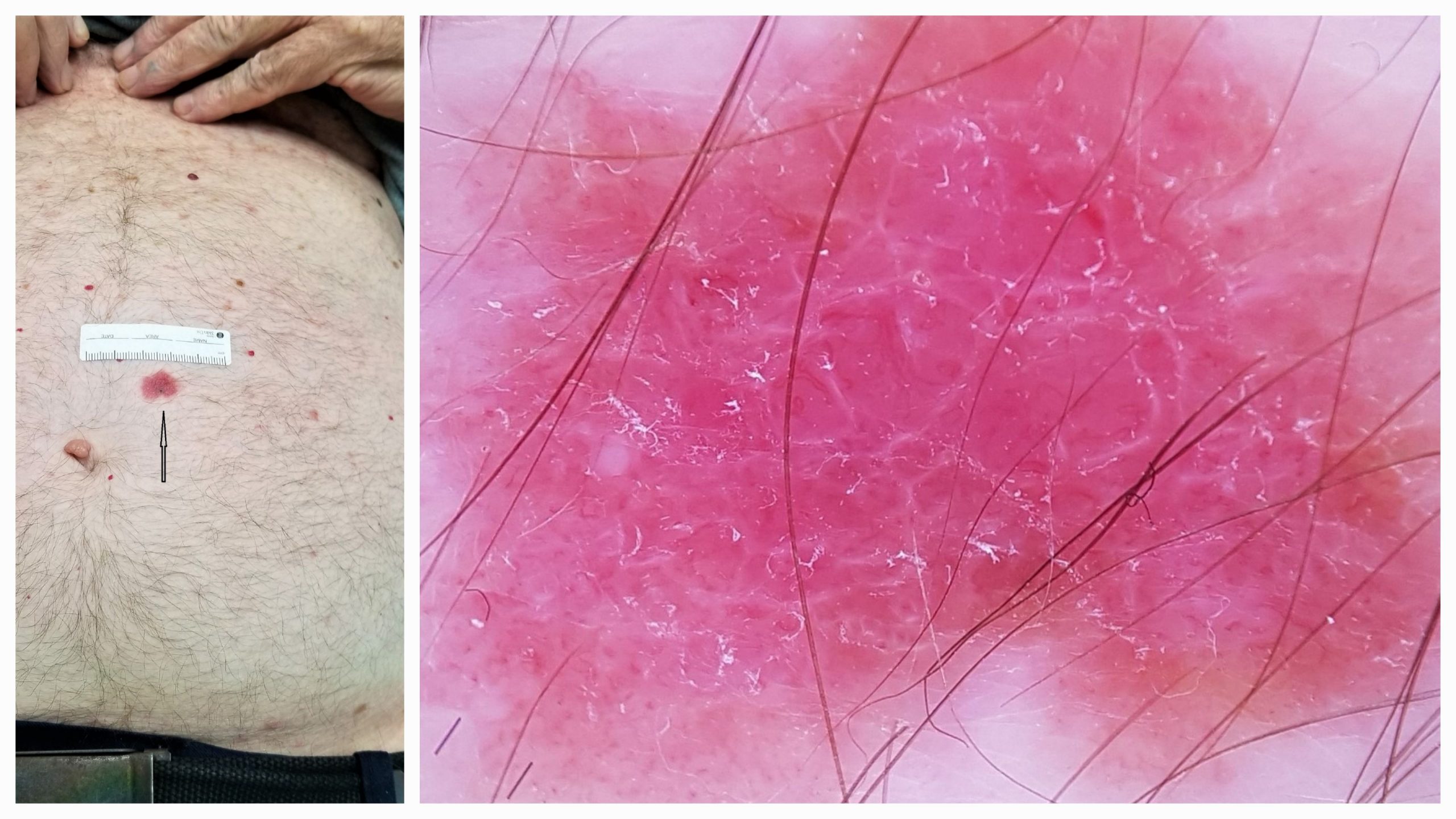
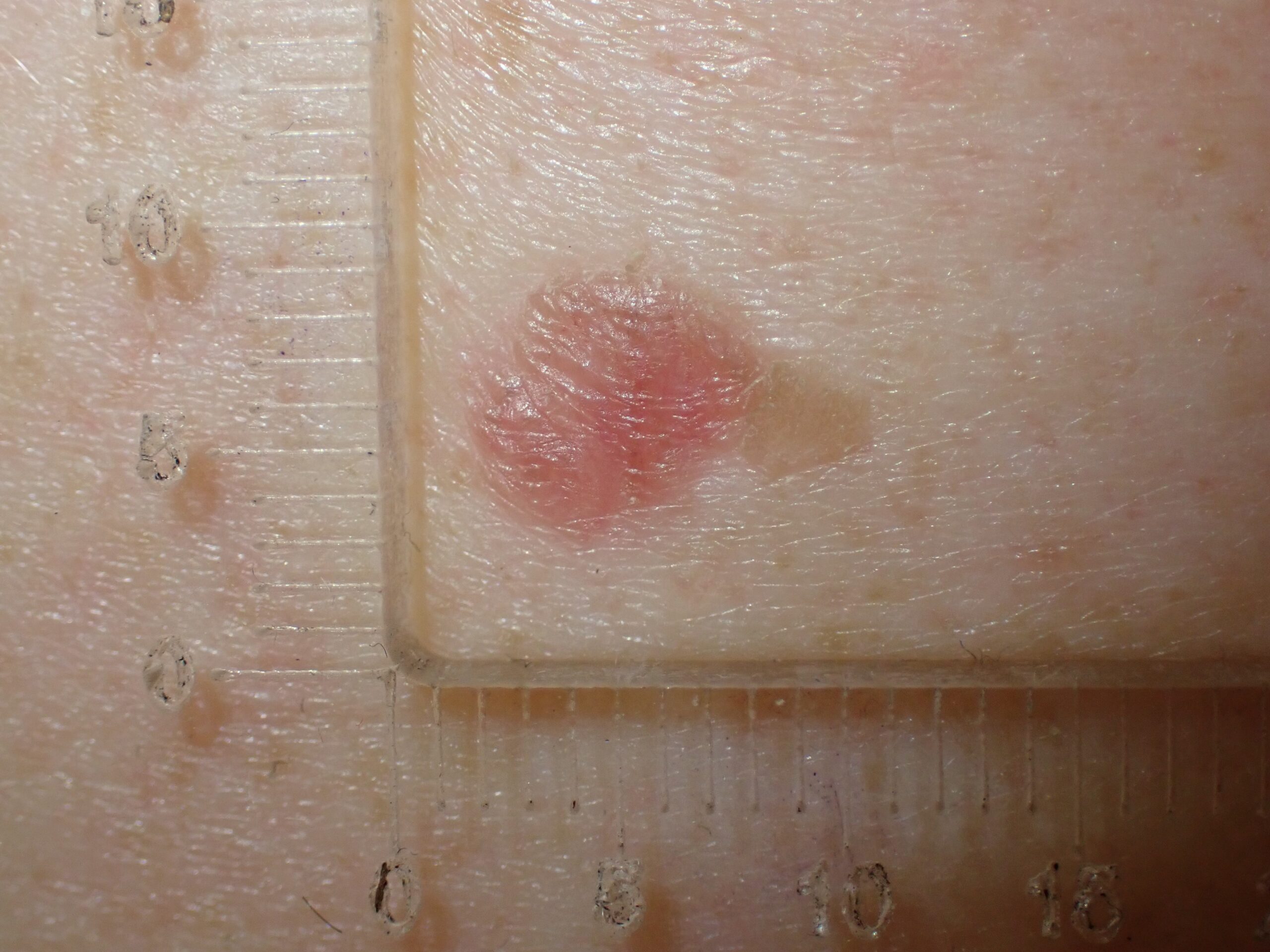
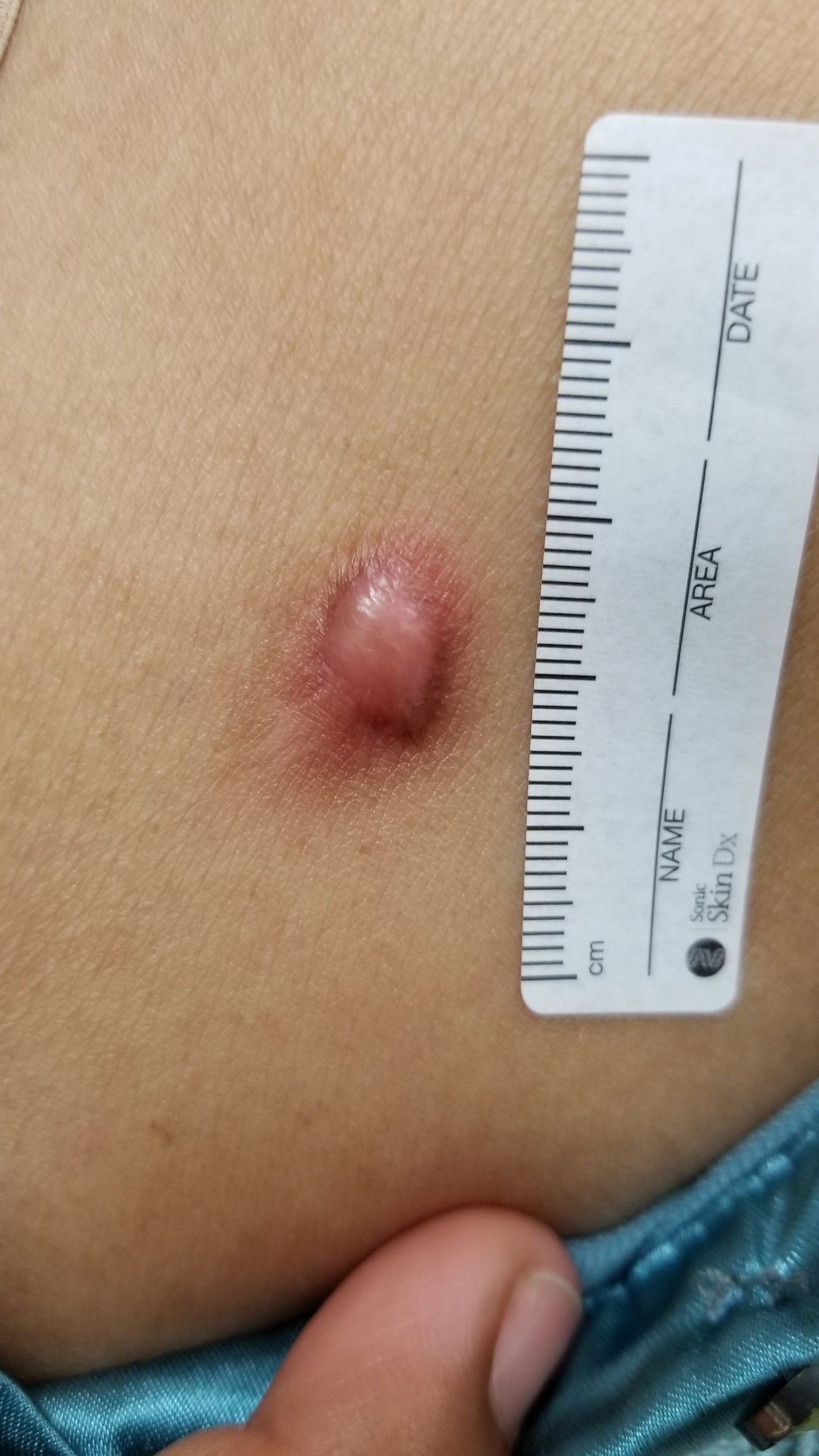
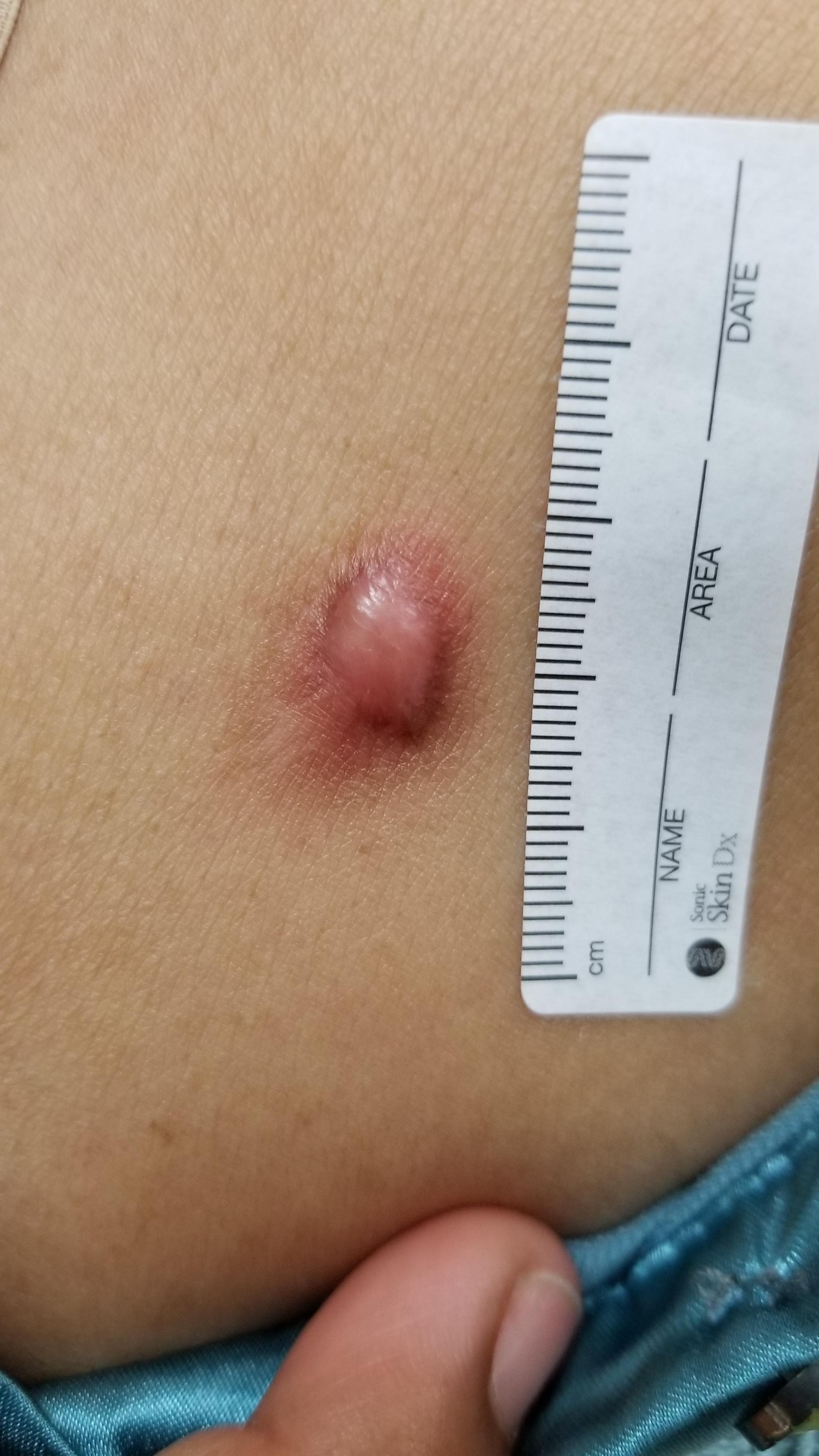
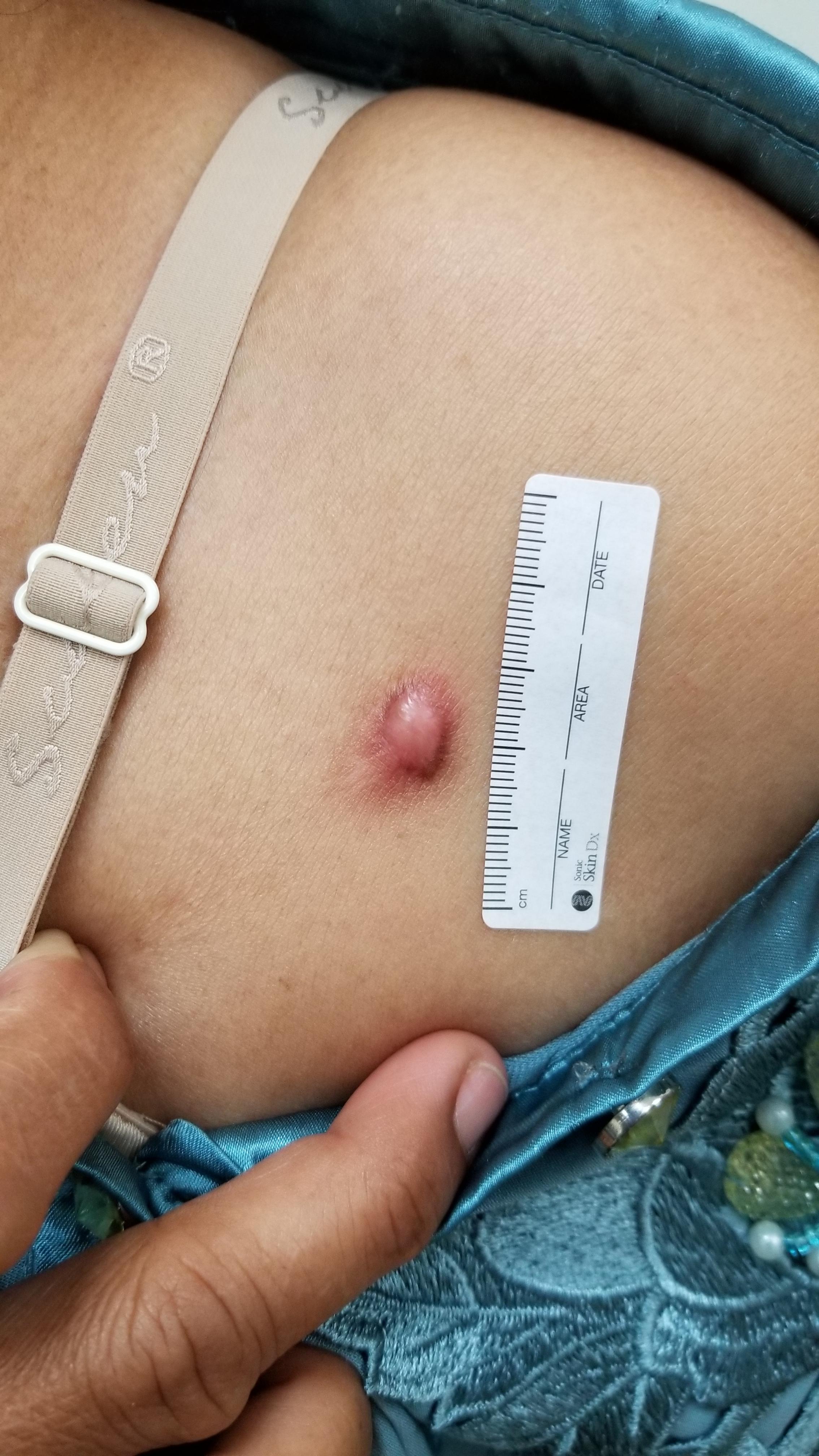
This week we revisit an engaging case from Dr Tim Aung. A 55-year-old female presented with 1-2 years' history of slow growth of an asymptomatic, non-tender lesion on the upper chest. Please review the images.
What is your impression, what is the differential diagnosis, and (if you would biopsy) what technique would you use?


Update:
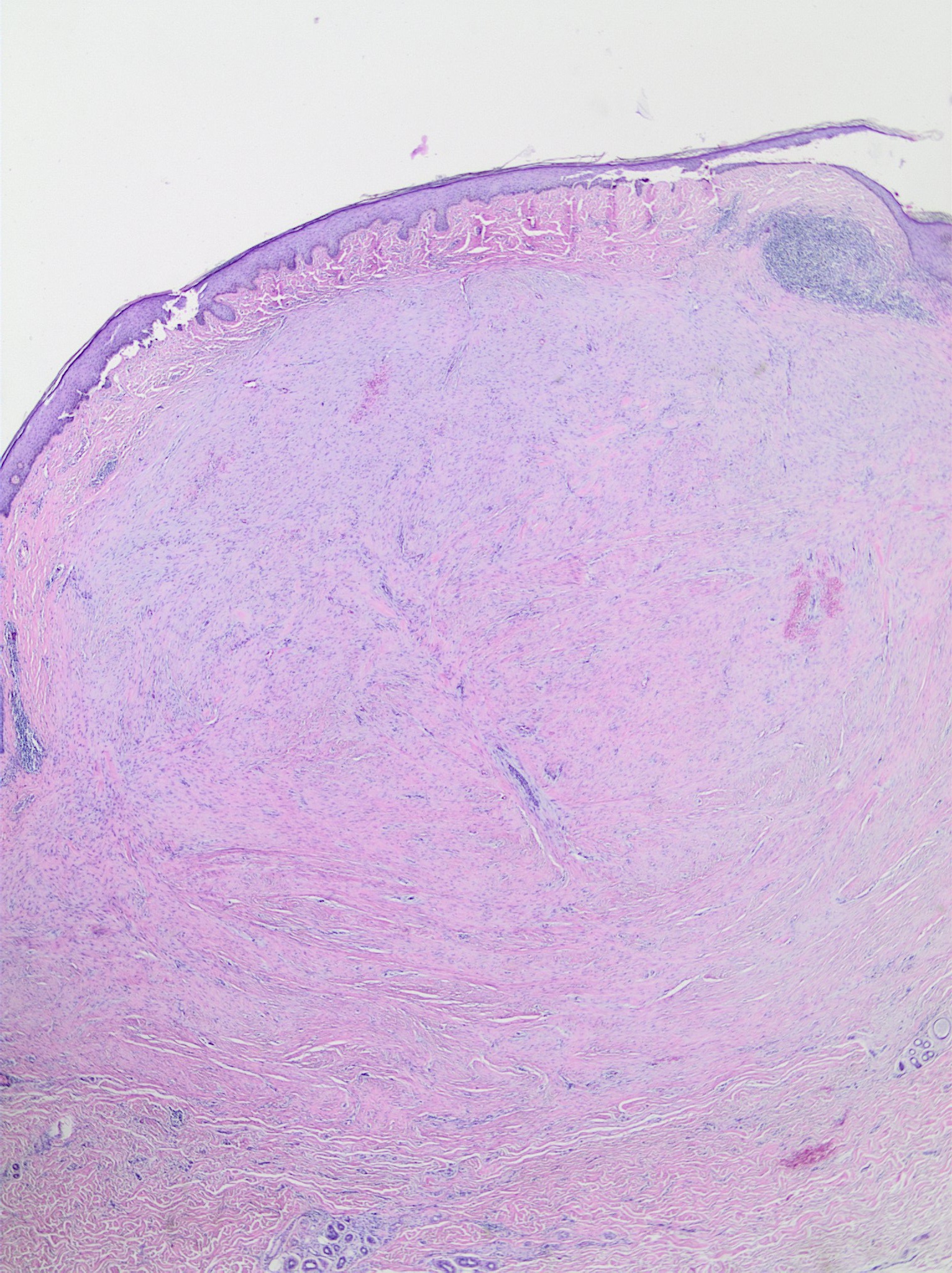
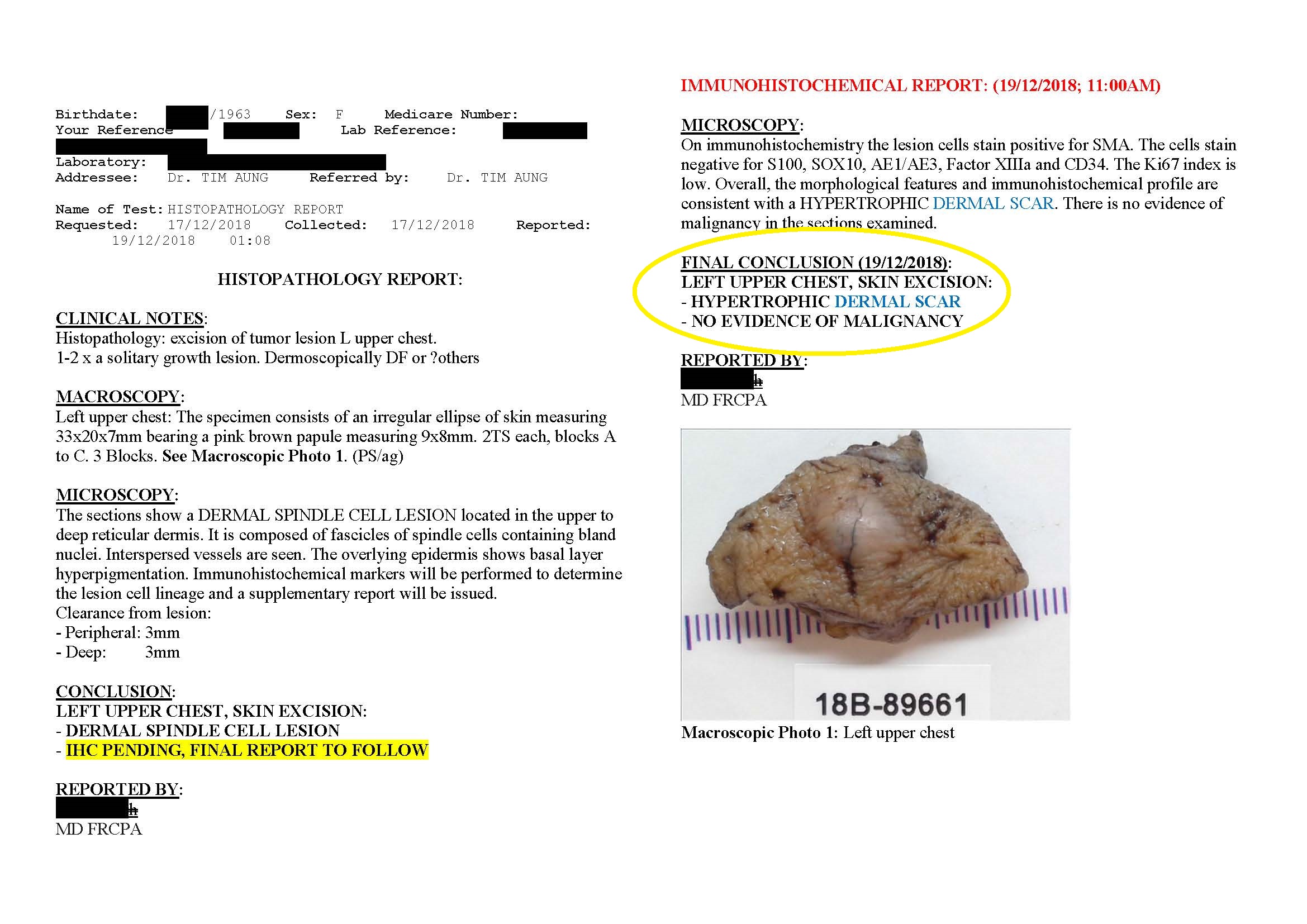
These are the results from the pathology report. What do you think now? How would you treat further?
– Prof David Wilkinson
We encourage you to participate in the case discussions and sumit your own clinical images and questions, so we can all learn together.
Comments