
 1800 867 1390
1800 867 1390In this case discussion from Dr. T. Harvey, we present a 34 year-old patient with an asymptomatic lesion on the left back. Please review the clinical and dermoscopy images.
Author
HealthCert Education
HealthCert Education
1 minute read
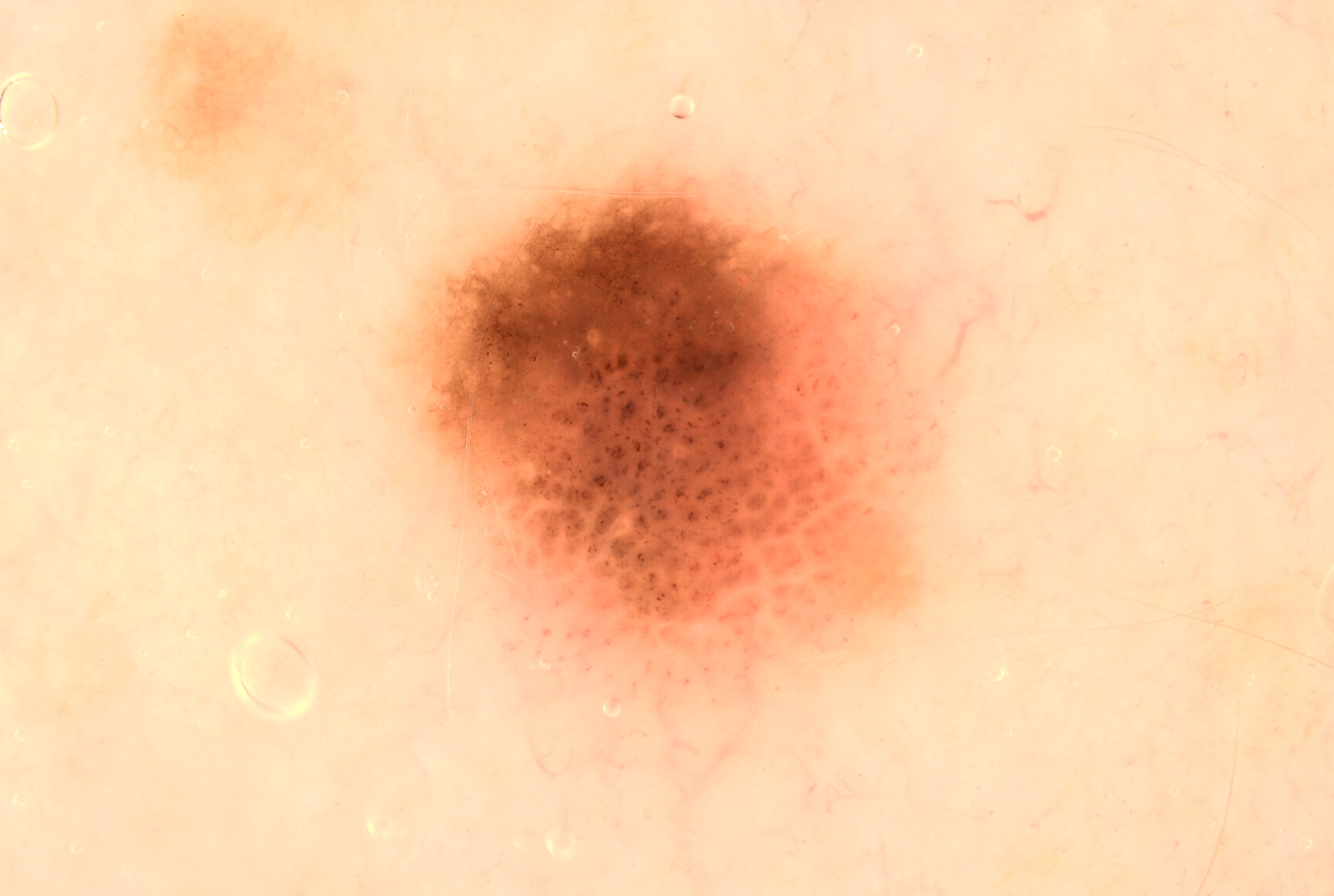
In this week's new case discussion from Dr Terry Harvey, we present a patient who came in for a routine skin check:
- 34 year-old male patient
- Asymptomatic lesion on left back
Please review the clinical and dermoscopy images. Any thoughts? What about the pigmented lesion noted? Specific thoughts on the dermoscopy?

![]()
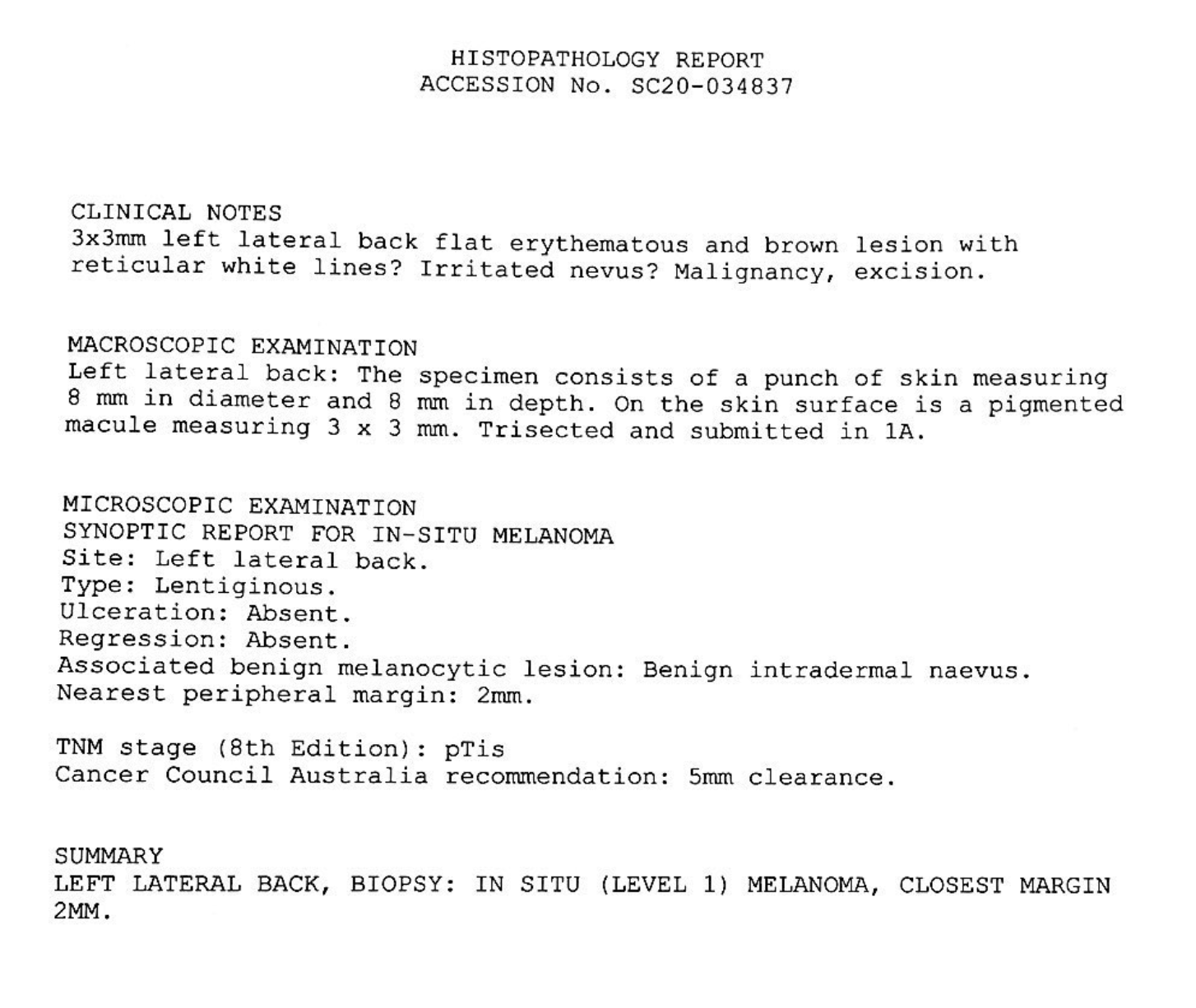
Update:
Here is the pathology result. What next?
We encourage you to participate in the case discussions and submit your own clinical images and questions, so we can all learn together.
Learn more about skin cancer medicine in primary care at the next Skin Cancer Certificate Courses:

Comments


