1800 867 1390
1800 867 1390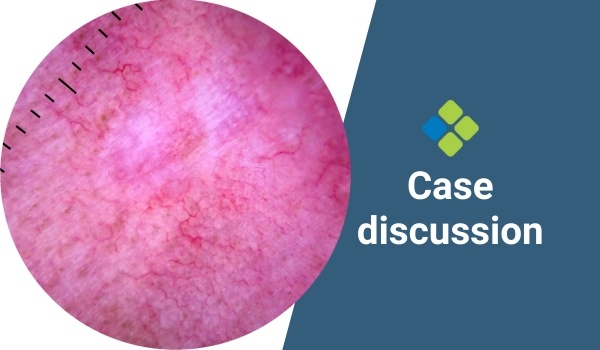
1 minute read
How would you manage this scar-like lesion on the face?
Case discussion: A 43-year-old lady presents with a scar beside her nose that she says was a sore she picked at until it finally healed. What do you think?