
 1800 867 1390
1800 867 1390
1 minute read
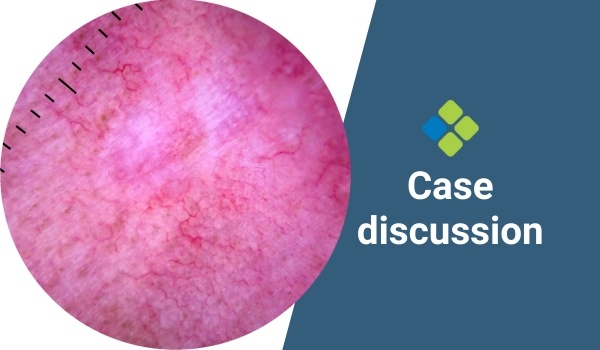
How would you manage this lesion on the lower back?
Case discussion: A 72-year-old male presents with a lesion on his lower back. What do you think?
Case discussion: A 72-year-old male presents with a lesion on his lower back. What do you think?
Case discussion: A 43-year-old lady presents with a scar beside her nose that she says was a sore she picked at until it finally healed. What do you think?
Profs Giuseppe Argenziano and Aimilios Lallas explore a series of challenging skin cancer cases they have encountered in their practice.

Read more about heat rash and its management in primary care, including assessment, diagnosis, and treatment.

Case discussion: 20x17mm pigmented lesion on anterior leg of 70-year-old man. Growing over years, with new raised area centrally. What do you think?

Read more about how to manage athletes with acute musculoskeletal injuries acquired from sport, including treatment protocols and psychological support.